Although exercise physiology has traditionally assumed that factors other than breathing limit exercise capacity, recent literature suggests that the respiratory system may indeed limit performance in highly trained athletes. We outline the remarkable capabilities as well as the potential limiting factors of the respiratory system, based on Dempsey’s article: Is the Healthy Respiratory System Built Just Right, Overbuilt or Underbuilt to Meet the Demands Imposed by Exercise?
(Dempsey et al.)
The respiratory system is highly adaptable and has enormous capacity. In young and less trained athletes without symptoms, breathing does not limit exercise performance. However, this is different for highly trained athletes or those experiencing symptoms.
Ventilation (VE):
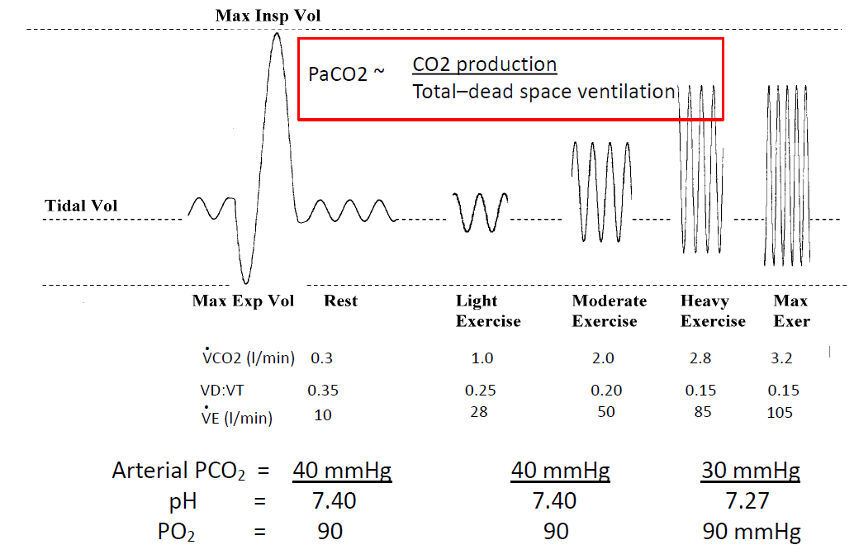
The respiratory system is designed to maintain constant oxygen and carbon dioxide concentrations in the blood under all circumstances. During exercise, ventilation increases both to supply more oxygen and to expel more CO₂.
Breathing mechanics:
As exercise intensity increases, the lungs must ventilate more air in accordance with energy demands and CO₂ production. To increase air intake per minute, either the depth of breathing (tidal volume, TV) increases, or the lungs breathe in and out more quickly (breathing frequency, Bfr). The tidal volume can only increase if exhalation becomes deeper, reducing the end-expiratory lung volume (EELV). The decrease in EELV and increase in TV are crucial for breathing efficiency. If EELV does not decrease sufficiently and TV does not increase adequately, breathing frequency rises more rapidly, disrupting efficient breathing mechanics. A too-rapid increase in breathing rate can significantly impact exercise capacity and may contribute to physical or mental symptoms.
Respiratory muscles:
The diaphragm and other respiratory muscles are well adapted to their task during intense exercise. These muscles do not fatigue easily. During strenuous efforts, additional muscles in the neck and chest assist the diaphragm. Expiratory muscles help forcefully exhale air, reducing EELV and allowing inspiratory muscles to lengthen, which increases their strength.
Pulmonary blood flow:
Numerous blood vessels surround the alveoli, with very thin walls to facilitate oxygen transport from the alveoli to the bloodstream and CO₂ transport from the blood to the alveoli. These vessels are also highly elastic, enabling a threefold increase in blood flow through the alveoli during maximal exertion compared to resting conditions.
Gas exchange:
As exercise intensity rises, more oxygen must be transported into the bloodstream, and more CO₂ must be expelled. The lungs ventilate more air to increase oxygen pressure in the alveoli. However, exercise-induced hyperventilation can sometimes lead to blood acidification, reducing oxygen binding to red blood cells (Bohr effect).
Potential limitations of the respiratory system in highly trained athletes:
Highly trained athletes require excessive air ventilation, leading to increased pressure in the chest and abdomen, which can cause several limiting factors:
Hyperinflation:
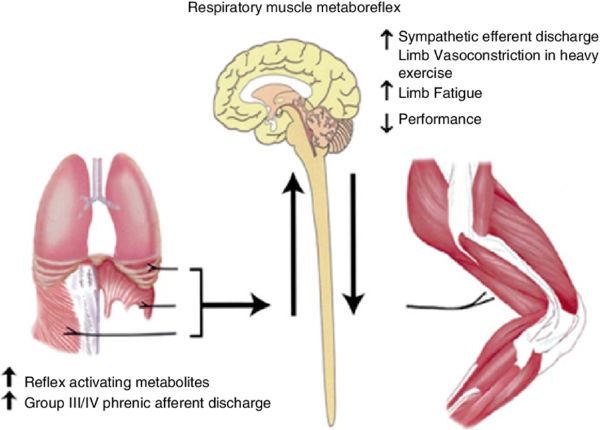
When inhaling and exhaling excessively, the balance between tidal volume and breathing frequency can become disrupted, causing excessively rapid breathing and insufficient exhalation time. This raises EELV, forcing the lungs to retain extra air and operate at a higher lung volume (LOV). This hyperinflation negatively impacts respiratory muscle function, causing them to work from a disadvantageous position. As a result, these muscles fatigue more quickly, consuming extra oxygen and blood that would otherwise be available for arm and leg muscles. This phenomenon is known as the respiratory metabolic reflex.
Respiratory metabolic reflex
Breathing muscles:
Expiratory muscles cannot simply work harder because excessive exhalation can collapse the flexible airways, trapping air inside and further increasing EELV, leading to hyperinflation. Additionally, inspiratory muscles use only 5–10% of their maximum strength during maximal exertion.
Reduced heart filling:
The high ventilation demand in well-trained athletes increases pressure in the chest and abdomen, affecting the heart’s ability to fill with blood. Reduced filling results in lower blood output from the heart.
Airway narrowing (EIB):
Exercise-induced bronchoconstriction (EIB) mainly occurs immediately after intense, sustained exercise. It is common in highly trained athletes, though its exact impact on performance is unclear. Frequent intense lung use can cause minor airway damage, increasing airway sensitivity and leading to narrowing in response to specific triggers. Another cause of airway narrowing is dehydration due to excessive ventilation.
Vocal cord closure (EILO):
The airway near the vocal cords is the narrowest part of the respiratory tract and naturally creates resistance to incoming airflow. Ideally, the muscles that open the vocal cords become more active during exercise. However, the narrowed airway increases airflow speed, sometimes pulling the vocal cords inward (Bernoulli’s principle), leading to exercise-induced laryngeal obstruction (EILO). EILO is associated with breathlessness, stridor, increased breathing effort, and heightened respiratory drive. This primarily becomes an issue when breathing frequency rises significantly.
Exercise-induced impairment in gas exchange (EIAH):
EIAH significantly contributes to muscle fatigue in the arms and legs, potentially reducing VO₂ max by up to 15%. In 30–70% of highly trained endurance athletes, oxygen levels decrease during intense exertion, with arterial oxygen saturation dropping by 4–12% and arterial oxygen pressure by 10–30 mmHg. These athletes exhibit a mismatch between alveolar ventilation and pulmonary blood flow, along with a limited hyperventilation response. Proper alveolar ventilation and pulmonary blood perfusion are crucial for adequate oxygen transport into the bloodstream. Studies indicate that reduced blood oxygen concentration negatively affects muscle fatigue and exercise capacity.
Respiratory muscle capacity:
Highly trained athletes tend to have stronger respiratory muscles that resist fatigue better. However, the diaphragm can experience fatigue when exercise intensity exceeds 80% of maximum capacity or when hyperinflation occurs. Once respiratory muscles fatigue, they divert blood and oxygen away from limb muscles via the respiratory metabolic reflex, reducing arm and leg performance.
Differences between men and women:
Dempsey suggests that women are more frequently and rapidly limited by their respiratory system than men. Women generally have smaller lung volumes and narrower airways relative to their body size, along with a lower gas exchange capacity. They also experience airflow limitations and reduced hyperventilation responses more quickly than men. Additionally, women require greater breathing effort, consuming more oxygen and experiencing breathlessness sooner. EIAH is more common in women and occurs at a much lower oxygen uptake capacity than in men